
CMS EDE marks a major step forward in healthcare data exchange. The audit submission window starts April 1, 2025, and runs through July 1, 2025, ending at 3:00 AM ET for interested entities. Healthcare organizations should plan ahead since building and auditing an EDE environment takes time – often a year or more.
Enhanced Direct Enrollment lets approved entities such as Qualified Health Plan issuers and web-brokers host Exchange coverage applications on their websites. This setup matches CMS’s bigger picture of a connected ecosystem. Patients can access their health records easily, providers get vital data when treating patients, and digital tools offer tailored support. The CMS EDE pathway gives cms ede partners new opportunities to join this evolving digital world while they manage to keep proper data exchange standards.
This piece dives into the key parts of data flow and PII mapping that HealthTech issuers need for CMS EDE work. It also covers compliance rules, security protocols, and ways to implement what cms approved ede partners must know about this federal initiative that shapes electronic health data exchange.
PII Access and Identity Verification in the CMS EDE Framework
Identity verification is the life-blood of the CMS Enhanced Direct Enrollment (EDE) framework. EDE entities use resilient identity management protocols to process sensitive healthcare information securely while managing to keep patient privacy intact. Here’s what you need to know about this framework’s most important components.
IAL2 and AAL2 Credential Requirements
The CMS EDE pathway requires specific identity standards from the National Institute of Standards and Technology (NIST). Identity Assurance Level 2 (IAL2) forms the foundation of identity proofing within the framework. You can verify this either remotely or in person. CMS approved EDE partners must build systems that verify applicants own the identities they claim.
Applicants must provide these specific combinations of evidence to meet IAL2 requirements:
- One Superior/Strong piece of evidence (if the issuing body verified the identity with two pieces of Superior/Strong evidence and the credential service provider checks with the issuer), or
- Two Strong pieces of evidence, or
- One Strong piece and two Fair pieces of evidence
The Authentication Assurance Level 2 (AAL2) standard requires proof that users control two different authentication factors through secure protocols. This layered approach will give a high level of confidence that people accessing CMS EDE systems are who they claim to be before they handle sensitive health information.
Digital Identity Verification via CMS-Approved Services
DE entities must verify identities of all consumers before submitting applications to the Federally-facilitated Exchange (FFE). Failed identity checks require entities to route consumers to either the traditional DE double-redirect pathway or send them to HealthCare.gov or the Marketplace Call Center.
Entities can choose from these verification services:
- Remote Identity Proofing/Fraud Solutions Archive Reporting Service (RIDP/FARS)
- Third-party identity proofing services that are Federal Identity, Credential, and Access Management (FICAM) Trust Framework Solutions (TFS)-approved
CMS improved its verification requirements. Consumers must now prove their identity before accessing the EDE environment. They can create only one account, and information must match across account creation, identity proofing, and eligibility application sections.
Agents and brokers must use multi-factor authentication that meets NIST standards. Manual consumer ID proofing processes need an EDE Entity-initiated Change Request approved by CMS before implementation.
Patient Consent and Disclosure Restrictions
Patient consent management plays a vital role in the CMS EDE framework. Consumers using an EDE Partner’s website must agree to the collection and transmission of their personally identifiable information (PII). This data often includes sensitive details like Social Security Numbers, date of birth, photographic identifiers, and health status information.
On top of that, agents, brokers, and web-brokers must follow strict rules about using and sharing consumer PII or protected health information (PHI). They must keep consent records for at least 10 years and show them during CMS monitoring, audit, and enforcement activities.
PII usage beyond authorized functions needs explicit consent from consumers or their representatives. CMS EDE partners cannot sell or share consumer PII submitted to or received from the FFE.
Patient priorities in transactions must reach all involved parties, including treatment cases. Laws and policies require respecting these priorities, including a patient’s right to limit their information sharing.
CMS approved EDE partners must state the purpose of all queries (like individual access, treatment, payment, or healthcare operations) to ensure legal compliance with disclosures.
Provider and Issuer Access to PII via EDE Pathway
The safe sharing of personally identifiable information (PII) is the foundation of the CMS Enhanced Direct Enrollment (EDE) pathway. Trust begins with identity verification, after which authorized entities can access patient information through well-laid-out methods. This access works through a carefully coordinated system that balances data availability with privacy protections.
CMS National Provider Directory Validation
The CMS National Provider Directory stands as the main source to verify healthcare providers who want access to patient information through the EDE pathway. CMS requires that any provider asking for patient data must be active in this directory. This verification step serves as a vital checkpoint that protects the whole data exchange system.
CMS yearly reviews compare the accuracy of covered plans’ machine-readable provider data files with online provider directories and other sources like the National Plan and Provider Enumeration System (NPPES). Recent reviews from 2017-2021 showed that only 28 percent of provider information from plans matched the NPPES registry data. This gap shows why we need one central, authoritative directory.
A national directory creates a single entry point for provider information updates instead of scattered directories across many systems. This approach helps prevent wrong information from spreading when providers change locations or other details.
Delegated Access for Issuers and Brokers
The CMS EDE system supports a delegated access model for issuers and brokers. Providers can use any application or delegated technology vendor/partner they choose to carry out transactions in the network. These delegated entities work as business associates under HIPAA rules and must have signed Business Associate Agreements.
The system treats these delegated actions just like direct provider actions. They work the same way from an authorization standpoint. In spite of that, delegated vendors or partners don’t have to provide reciprocation in the network unless their contracts say otherwise.
Enhanced Direct Enrollment partners can collect consumer information and send it to CMS as the operator of the Federally-facilitated Exchange (FFE). This happens only after getting specific consent from the consumer. The FFE then uses this PII to determine if people qualify for insurance affordability programs, including QHP enrollment, Medicaid, CHIP, and premium tax credits.
Use of PII for Treatment and Payment Purposes
The system sets clear rules for using PII based on purpose. Providers must meet three conditions to get complete patient information: they need an identity-verified credential (IAL2/AAL2 equivalent), verification in the CMS National Provider Directory, and confirmation of treatment purposes. All nodes must then share what they know about the patient, except where laws restrict it. This full access recognizes why complete information matters for treatment decisions.
Every query must state its purpose, whether for individual access, treatment, payment, or healthcare operations. This documentation keeps all information sharing legal and appropriate.
The FFE can also use PII for program support tasks such as:
- Plan Management
- Eligibility and Enrollment (including appeals integration)
- Financial Management activities
These tasks include using contact details like email addresses and phone numbers to reach consumer applicants about applications, QHP coverage, or related issues. The EDE Partner Agreement bans selling or sharing consumer PII submitted to or received from the FFE, which protects data integrity throughout the system.
Data Standards for PII Exchange in EDE Systems
The CMS EDE pathway needs standard ways to exchange data. Organizations working with CMS must follow specific technical standards about how they structure, store, and send protected health information. These standards will give a consistent way for healthcare systems to work together.
USCDI v3 Compliance for PII Fields
The United States Core Data for Interoperability Version 3 (USCDI v3) forms the foundation for PII exchange in CMS EDE systems. This standard set of health data classes creates a common framework that works nationwide. The number of required elements in v3 has almost doubled compared to the last mandatory version (USCDI v1).
Every CMS EDE partner must comply with USCDI v3 by January 2026. This rule substantially expands the standardized data elements they need to capture and share:
- Patient demographics and identifiers
- Clinical notes and assessment information
- Insurance coverage details
- Care team members and relationships
- Health concerns and goals
- Diagnostic imaging and laboratory results
USCDI v3 plays a crucial role in PII exchange by including detailed terminologies for each data class. This ensures systems can understand each other. Organizations that don’t map these data classes correctly face heavy penalties—up to $1 million per patient for wrong mapping or missing data.
FHIR API Requirements for Structured Data
CMS EDE pathway requires FHIR (Fast Healthcare Interoperability Resources) APIs to exchange structured data. Networks must provide data access using FHIR APIs that follow the US Core FHIR implementation guide. This guide sets minimum constraints on FHIR resources to create standard profiles.
FHIR Release 4.0.1 introduces the first set of normative FHIR resources that define core health data’s content and structure. CMS approved EDE partners must build FHIR-based API platforms that support:
- US Core FHIR profiles as the foundational requirements
- Full FHIR capabilities statements
- USCDI V3 with proper terminology compliance
- FHIR Bulk data exchange capabilities to reduce system stress
These FHIR standards don’t just make systems work together—they solve a key business challenge: making data from different sources consistent. One expert explains, “A payer gets information from multiple sources… As a payer, we have to ensure we provide concise and clear information back through the API”.
The CMS Interoperability and Patient Access Final Rule (May 1, 2020) requires payers to use these APIs. This improves how healthcare data moves between systems, whether sharing with patients or exchanging between payers and providers.
Machine-Readable Formats for Clinical Documents
Clinical documents in the CMS EDE framework must follow standard, machine-readable formats. Chart notes and clinical documents (including radiology reports, scanned labs, and specialist notes) need both machine-readable and human-readable versions as USCDI v3 specifies.
The system supports PDF, TIFF, and JPG formats for human reading. These documents must also work as FHIR attachments for automated processing. This two-format approach lets both human clinicians and computer systems use the information effectively.
Clinical Document Architecture (CDA) adds another important standard that uses XML markup to define document structure. CDA includes:
- Headers containing document metadata
- Body content with structured narrative blocks
- Terminology standards like LOINC or SNOMED CT to improve semantic interoperability
The Consolidated CDA (C-CDA) implementation guide brings multiple document types into one standard. This creates a foundation for consistent document sharing across the CMS EDE pathway. Following these standards helps CMS EDE approved partners stay compliant with federal rules while getting the most from their data.
Real-Time Data Flow and PII Query Handling
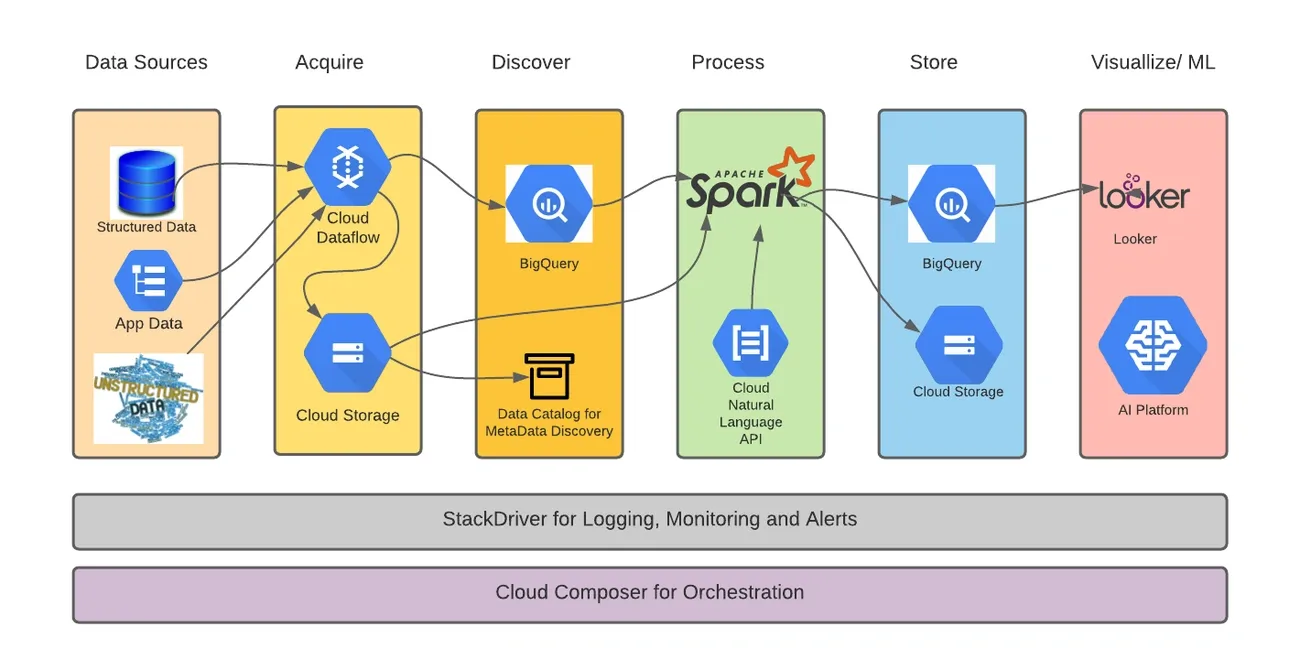
Image Source: Pluto7
The CMS EDE ecosystem’s success depends on quick data exchange between partners and federal systems. The Enhanced Direct Enrollment pathway needs instant communication to give users a smooth experience on partner websites. This approach helps maintain data integrity across all systems.
Timely Response Expectations for EDE APIs
A sophisticated suite of application programming interfaces (APIs) powers the CMS EDE pathway. These APIs enable instant communication between authorized entities and federal systems. Primary EDE entities need to work with more than 20 different APIs that aid eligibility determination, enrollment, and post-enrollment activities. Consumer information flows securely through these bidirectional channels to the Federally-facilitated Exchange (FFE) and back to the EDE entity‘s website.
The FFE platform processes API requests right away. It applies the same business logic and workflow that HealthCare.gov uses to make determinations. The system puts all information through similar data verification and validation routines as direct human input on the federal platform.
CMS EDE partners need responsive systems that can:
- Show eligibility results right after FFE processing
- Support instant enrollment confirmation
- Allow immediate post-enrollment actions like plan changes or information updates
Record Locator Services for PII Discovery
The CMS EDE framework has advanced record location features that help authorized users find relevant PII in different systems. Administrators and authorized users can get consumer records from the Marketplace Consumer Record (MCR) system using:
- First and last name
- Date of birth
- Social Security Number
- Geographic identifiers (state, city, zip code)
- Email address
These record locator services start the search functions and are the foundations of PII within the MCR system. Health Insurance Marketplace call center representatives utilize these services to find relevant records faster and solve customer issues.
Record discovery features help spot and fix enrollment issues more quickly. This optimized approach helps with daily customer service tasks and special functions like appeals processing.
Query Logging and Audit Trails
Detailed audit trails are vital security components because of the sensitive nature of personal information in the CMS EDE pathway. The framework needs specific logging requirements to monitor, analyze, investigate, and report system activity.
Each query in the CMS approved EDE partner ecosystem must create audit records with:
- Date and time of the event
- System component where the event occurred
- Type of event and outcome (success or failure)
- User identity
- Execution of privileged functions
The system tracks extra events for privacy monitoring:
- System access attempts (successful and unsuccessful)
- Attempts to create, read, write, modify or delete extracts containing PII
- Privileged activities or system-level access to PII
- Concurrent logons from different workstations
Organizations must keep these audit records online for at least 90 days and store them offline for 10 years. This helps with investigations and meets regulatory requirements. CMS EDE approved partners must check these records weekly for unusual activity. They should adjust review frequency based on risk factors or credible threat intelligence.
These careful audit practices protect PII as it moves through the complex systems of the CMS EDE ecosystem.
Security and Trust Requirements for PII Handling
A strong security framework behind CMS EDE operations provides strong safeguards for sensitive health information. Multiple safeguards work together to keep patient privacy and system integrity safe as personal information flows through the ecosystem.
HITRUST Certification for CMS EDE Partners
CMS requires HITRUST certification as the gold standard for all cms ede partners. The CMS Interoperability Framework will need validation equivalent to HITRUST certification starting July 31, 2025. This requirement goes beyond a simple compliance checkbox and represents a detailed approach to protect healthcare data through specific controls and thorough assessment.
HITRUST framework makes compliance easier by combining multiple standards into one model. CMS approved ede partners get two benefits: they meet CMS requirements and advance their HIPAA compliance obligations. The certification process reviews three significant safeguard categories:
- Administrative protections (policies, procedures, training)
- Physical controls (facility access, workstation security)
- Technical measures (encryption, authentication, monitoring)
HITRUST certification helps organizations using the cms ede pathway build trust with patients, providers, and regulators by showing real security commitments instead of theoretical policies.
Access Control and Consent Enforcement
Along with certification standards, the cms ede framework has clear requirements for consumer consent before handling PII. We needed agents, brokers, and web-brokers to get and document consent before:
- Collecting or using any consumer PII to provide Marketplace coverage quotes
- Assisting with enrollment in Qualified Health Plans
- Helping consumers apply for advance payments of premium tax credits
This documentation must be managed to keep for 10 years and shown when asked during CMS monitoring, audit, and enforcement activities. Lead generators and other third-party methods are not valid ways to get consent.
EDE partners must give consumers a chance to explicitly opt-in for PII collection, creation, disclosure, access, maintenance, storage, and use. Consumers should also have ways to limit how their information is used. PII cannot be used beyond authorized functions without explicit consent from the consumer or authorized representative.
Audit Logs for Identity and Authorization Events
Detailed audit logging forms the foundation of accountability in the cms ede security framework. Each logged event must show key details at a glance:
- Date and time of the occurrence
- Service that logged the occurrence
- Category and name of the activity
- Status of the activity (success or failure)
Organizations need to keep these audit logs online for at least 90 days and archive them offline for 10 years to help with investigations and meet regulatory requirements. CMS ede partners must review these records weekly to spot unusual activities.
Systems must log additional details for privileged actions, especially those with consumer PII. Events needing special monitoring include system access attempts, attempts to change PII, privileged activities affecting PII, and concurrent logons from different workstations.
CMS can immediately stop an EDE Partner’s authorization to collect, use, or share information from Exchange applicants if serious misconduct with PII happens. This right to terminate applies when partners fail to properly use or secure PII. This highlights why strong security practices matter throughout the cms ede ecosystem.
CMS Aligned Network Responsibilities for PII Exchange
Participation in the CMS EDE ecosystem entails specific network-level obligations for handling personally identifiable information. These requirements extend beyond individual entity responsibilities to ensure system-wide transparency and accountability throughout the data exchange process.
Publishing PII Access Metrics in CMS Directory
Networks operating within the CMS EDE pathway must regularly publish comprehensive metrics regarding PII access and usage. Altogether, these networks agree to provide statistics on network queries, including counts of successful and unsuccessful replies. This data transparency enables CMS to develop performance scorecards based on network metrics and user feedback.
Though these requirements may seem administrative in nature, they serve a vital purpose: enabling healthcare entities to make informed business decisions with the best available information. As one industry document notes, “reduction in information asymmetry will ensure that payers, providers, and employers are able to interact on a level playing field”.
Initially, cms ede partners must establish automated systems to track these metrics and prepare them in formats specified by CMS for inclusion in the National Provider Directory.
Inter-network PII Query Support
The CMS Interoperability Framework mandates that all networks implement “standards-based inter-network connectivity”. Hence, cms ede approved partners must support the ability to query and respond across federated networks using widely accepted query formats and protocols.
Networks must furthermore enable searching capabilities for patient records, including:
- Network-wide searches for all records of a patient
- Targeted queries for records in specific geographic areas or from particular NPIs
For cms ede pathway implementation, this interconnected approach reduces duplicative data collection efforts. Till all networks achieve full compliance, CMS has proposed measuring the administrative burden of provider information collection and submission over time to demonstrate whether the system achieves its intended outcomes.
Transparency in Endpoint and Participant Listings
Data networks within the CMS EDE ecosystem must maintain complete transparency regarding their participants and technical endpoints. Undeniably, these networks “agree to be displayed as a CMS Aligned Network and to publish membership information, NPI level participants, relevant endpoints and other inter-connected networks in the CMS National Provider Directory”.
This transparency obligation extends to maintaining updated information about providers. Thus, when networks discover new information about providers—such as contact details, license information, interoperability endpoints, or insurance plans accepted—they must promptly update the CMS National Provider Directory.
CMS further stipulates that data networks recognized as CMS Aligned Networks must adhere to FHIR API requirements and USCDI standards. Throughout this process, networks maintain the responsibility to update provider directory information in the format and cadence established by the agency.
HealthTech Issuer Responsibilities in PII Mapping
HealthTech issuers in the CMS EDE ecosystem must handle specific PII mapping tasks. They need to pay close attention to documentation and data flow management. These entities must keep complete records of how personally identifiable information flows through their systems. This documentation supports the framework’s integrity.
PII Mapping to CMS Audit Toolkits
HealthTech issuers need to map their PII handling processes to CMS audit toolkits during the Enhanced Direct Enrollment audit. The audit has two main parts:
- Business Requirements Audit – checks if applications work correctly
- Privacy and Security Audit – makes sure PII protection systems work well
Each potential primary EDE Entity needs one or more independent Auditors. These auditors check and certify that websites and operations meet program requirements. The privacy monitoring system must track several events:
- System access attempts
- Attempts to create, modify, or delete PII extracts
- Privileged access to PII
Companies that want to join the CMS EDE pathway must go through an operational readiness review. This review needs full documentation of all PII touchpoints in their systems.
PII Flow Documentation for Upstream Entities
PII flow documentation is crucial for HealthTech issuers through the required Appendix B submission. This document shows all data connections, functionality, and systems between primary EDE Entities and upstream EDE Entities.
Issuers must document these details for each connection:
- Information being transmitted (PII data elements, enrollment information, eligibility details)
- Connection types used (IPSec VPN, SSL, Secure File Transfer, API)
- Data sharing agreements in place (including terms, parties, and protection requirements)
Issuers must keep clear records of consumer information flow between their environment and external EDE systems. They need to update this form yearly and when adding new upstream EDE Entities.
CMS EDE Approved Partners and Data Sharing Agreements
CMS keeps a public directory of all approved EDE entities as of December 2025. This list has issuers, web-brokers, and technology providers. These partners must sign formal agreements about PII handling.
The life-blood of these arrangements is the Enhanced Direct Enrollment Agreement with CMS. This agreement lets EDE Partners get informed consent from people who use their information. Issuers must use specific agreement types based on how they share information:
- Computer Matching Agreements (CMAs) – for federal agency disclosures
- Information Exchange Agreements (IEAs) – for PII sharing with HHS, federal agencies, or state agencies
- Data Use Agreements (DUAs) – for PII/PHI disclosures from CMS
Upstream entities using a primary EDE Entity’s environment must document their data protection safeguards. Hybrid, non-issuer upstream EDE Entities need separate privacy and security audits if they add more than minor branding changes.
Implementation Timeline and Early Compliance Steps
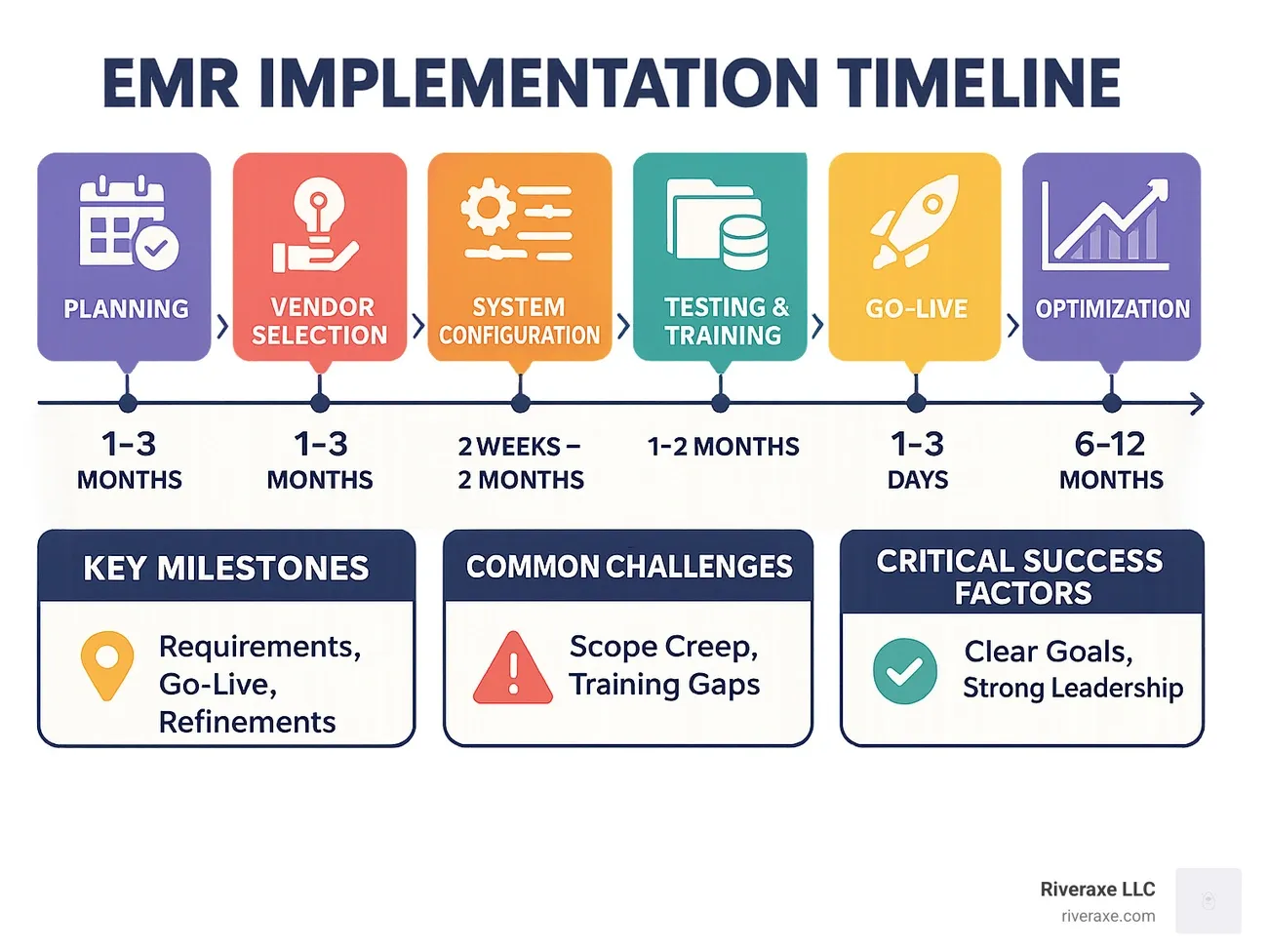
Image Source: RiverAxe
Getting ready for Enhanced Direct Enrollment needs specific timelines and preparation steps. Organizations must align their development work with CMS’s approval process.
Audit Submission Window: April 1 – July 1
The yearly cms ede audit submission period starts April 1 and ends July 1 at 3:00 AM ET. Organizations must submit complete audit packages before this deadline to qualify for the next year. Building and auditing an EDE environment takes significant time—often a year or more. Organizations should start their preparations early. Applications work best when they’re fully ready by February. This schedule gives teams enough time to work on CMS feedback, which usually takes two weeks or more.
Mini Audit and Functional Testing Requirements
The cms ede pathway needs two separate audit parts: a Business Requirements Audit and a Privacy and Security Audit. These reviews check both how the application works and how it protects PII. Teams must prepare all API, communications, and UI documentation carefully as these are key elements for a successful business requirements audit. Book a Readiness Call with compliance experts to get a full picture of your preparation status before submitting audit materials.
CMS EDE Entity Kickoff and Training Modules
After approval, cms ede partners must finish required training modules on the REGTAP platform (https://regtap.cms.gov/). Everyone taking the training needs to complete all course conclusion pages. While sending training proof to CMS isn’t needed, organizations should keep copies of completion pages for possible CMS checks. Teams must also maintain test environments that match their production systems and secure them with proper access credentials.
Conclusion
The CMS Enhanced Direct Enrollment pathway has changed the map of healthcare data exchange. It opens new doors for HealthTech issuers but demands strict standards for PII handling. Identity verification is the life-blood of this framework. Healthcare providers must meet IAL2 and AAL2 standards to access sensitive healthcare data. The National Provider Directory validation, delegated access models, and standardized data formats work together. They ensure secure information exchange throughout the ecosystem.
HealthTech issuers face technical hurdles with USCDI v3 compliance and FHIR API requirements. These need attention before the April 1-July 1 audit submission window. Companies should start early to map their PII handling processes to CMS audit toolkits. HITRUST certification is a must-have requirement that forms the foundations of all EDE operations.
A detailed documentation of data flow between primary entities and upstream partners makes implementation successful. Companies must create precise PII mapping that covers all data touchpoints in their systems. Organizations in the planning phase should Book a Readiness Call with compliance experts. This helps them assess their preparation level before creating audit materials.
Tomorrow’s healthcare data exchange needs a balance between continuous connection and resilient privacy protections. Setting up CMS EDE needs heavy investment in technical infrastructure and compliance programs. Yet it ended up creating a more connected healthcare ecosystem. Patients, providers, and payers all benefit from secure, standardized data exchange. Healthcare organizations that welcome these standards today will be ready for the regulatory changes of tomorrow.
Key Takeaways
Understanding CMS EDE’s complex data flow and PII mapping requirements is crucial for HealthTech issuers seeking to participate in this transformative healthcare data exchange ecosystem.
• Identity verification is mandatory: All CMS EDE participants must implement IAL2/AAL2 standards and obtain patient consent before accessing any personally identifiable information through the pathway.
• USCDI v3 compliance deadline approaches: Organizations must achieve full USCDI v3 and FHIR API compliance by January 2026, with penalties reaching $1 million per patient for incorrect data mapping.
• HITRUST certification becomes required: Starting July 31, 2025, all CMS EDE partners must obtain HITRUST certification to demonstrate comprehensive security controls for PII handling.
• Audit submission window is narrow: The annual audit submission period runs April 1-July 1, requiring organizations to begin development at least one year in advance for successful implementation.
• Comprehensive PII documentation is essential: HealthTech issuers must maintain detailed records of all data flows, connections, and sharing agreements between primary entities and upstream partners for CMS compliance.
The CMS EDE pathway represents the future of secure healthcare data exchange, but success requires early preparation, robust security frameworks, and meticulous attention to compliance requirements. Organizations that invest in proper implementation today will be positioned as leaders in the connected healthcare ecosystem of tomorrow.
FAQs
Q1. What is Enhanced Direct Enrollment (EDE) in healthcare? Enhanced Direct Enrollment is a service that allows approved health insurance issuers and web-brokers to enroll consumers in Exchange coverage directly through their own websites, without redirecting to HealthCare.gov.
Q2. What is the National Provider Identifier (NPI) and why is it important? The NPI is a unique identification number for covered healthcare providers. It’s crucial for administrative and financial transactions, serving as a standardized identifier in the healthcare system.
Q3. How does HealthSherpa utilize the EDE platform? HealthSherpa, as an EDE platform, enables clients to enroll in marketplace coverage without using HealthCare.gov. This service is available in all states participating in the federal exchange.
Q4. What are the key responsibilities of CMS EDE partners? CMS EDE partners are responsible for providing a complete Exchange application, shopping, and enrollment experience for consumers. They must adhere to strict security standards, maintain accurate documentation, and undergo regular audits.
Q5. When is the annual audit submission window for CMS EDE entities? The annual audit submission window for CMS EDE entities opens on April 1 and closes on July 1 at 3:00 AM ET. Entities must submit complete audit packages before this deadline to be considered for participation in the following year.